Working through the 110 interviews conducted to date (20 prisoners, 30 community members, 30 prisoner family members, 30 prison officers) by or for this research team has been a key aspect of my work with this project. These interviews were intended to draw out details of individual experience and understanding to help develop a well-rounded and carefully evidenced understanding of the Guyana Prison Service (GPS) as it operates today. This work is in support of our efforts to understand the historical roots and present-day operations and challenges of the GPS and more broadly, and specifically, issues around MNS in these systems and spaces.
Some interviews were conducted by members of the project team, but the COVID-19 pandemic interrupted this work. We were lucky to connect with Fiona (Magda) Wills, the Director of SSYDR who took over the interviews in Guyana, with great success. All interview participants gave their consent to be interviewed and audio recorded, for their contributions to be used anonymously by the project team, and generously shared their time, experiences, and impressions of the GPS. Interviewees were thanked with a small cash gift (honorarium).
Interviewing for this project involved connecting with people whose lives are intimately connected – directly and indirectly – with Guyana’s prisons. These can be difficult stories to share, as people revisit sensitive subjects and delicate moments. The experience of deep listening as an interviewer also involves an intensity of experience and emotion. To better understand the experience of interviewing family members of prisoners, people who live near prisons, and prison officers, we asked Fiona to tell us about her experience and she generously agreed to sit down with Clare Anderson and Emma Battell Lowman earlier this year.
We were keen to learn whether prisons were something people were interested in discussing. Fiona explained, “People generally, people are always very willing to talk, I find! […] they want to talk more, and a lot of it isn’t necessarily related to the interviews but they’re just happy to talk.” In some cases, it seems, these interviews offered a space for people to feel heard about their concerns and experiences with the prison system.
What stood out for Fiona across the three groups she interviewed – family members of prisoners, people who live near prisons, and prison officers – was that “they are all stakeholders” and were invested in the prison spaces being well-maintained and tidy as an important aspect of these persons’ mental health. Many interviewees identified the purpose of prisons as being for the rehabilitation of prisoners as part of a shift from a penal to a correctional approach in the GPS. As Fiona identified, “if you really want to rehabilitate, my belief is that you have to make everybody’s space liveable” and that means attending to the physical spaces inside and outside the prison to benefit the diverse communities involved in and impacted by Guyana’s prisons.
It was something more personal that Fiona told us had the biggest impact on her over the course of conducting the interviews. The thing that “jolted” her was the number of mothers she interviewed who had sons – particularly sons in their 20s – in the prison system who were impacted by the incarceration of their child, and often maintained narratives of their innocence. Fiona said this “gripped” her, because she also has a young son, and this connection made these experiences stand out.
Fiona’s team transcribed the audio recordings of the interviews with great care and expertise (good transcription is not easy or fast!), these were then sent securely to the UK-based project team, and that’s where I come in. I’m the most recent addition to the project team and have come on board to help as the project nears completion. The project team is an excellent collaboration between the University of Leicester and Leicester Prison Service in the UK, and the University of Guyana and Guyana Prison Service, which allows us to combine specific skills and expertise from several areas of study with on-the-ground experience and expertise in the GPS. In turn, this means the work we are doing stays closely tied to the needs and priorities of those most impacted by the GPS while also seeking to make contributions and changes to global research on prisons, carcerality, and MNS (mental, neurological, and substance use disorders). By working to analyse and prepare the interview transcripts for use by the research team, I help to support the collaborative work of the project team to produce practical materials for use in the GPS and research articles for public and academic audiences.
My work with the interview transcripts took place thousands of miles from Guyana, but created a sense of proximity and intimacy as I worked carefully through each one to identify themes and information connected with the project’s key questions and concerns. The immediacy of frustration of family members and prisoners at the long delays in moving cases forward in the justice system, the evident strain on family members who have to provide support to prisoners in terms of food, toiletries, and money to ensure a reasonable level of health, and the fear of violence spilling over from the prisons into the streets and homes of people who live nearby all came through powerfully in the words and stories on the page.
The emotional experience of working with these stories is an important aspect of our work – it helps us find empathetic connections with people whose lives and our own are quite different, and it helps us understand from a personal perspective the direct impacts of the prison system as it operates today in Guyana. Taken together, these interviews present a powerful picture of a system whose impacts extend far beyond the prison walls and the strong case for investment and improvement.
Dr Emma Battell Lowman is a research associate on the ESRC GCRF project Mental Health, Neurological and Substance Abuse Disorders in Guyana’s Jails, 1825 to the present day.
Interviews conducted at the Georgetown and Lusignan prisons in 2019 as part of a collaborative research on the topic of “Mental, Neurological and Substance Abuse disorders in Guyana’s Jails – 1825 to the Present Day” revealed that a number of mental health challenges (diagnosed and undiagnosed) are experienced by both prisoners and prison staff, with depression seeming to be the dominant one. Depression in the context of Guyana’s prisons, is exacerbated by several factors; limited recreational activities, poor or limited work and education rehabilitation programmes, and an absence of, or limited contact with family members to name a few.
Image: Lusignan Prison 2019, Professor Martin Halliwell, University of Leicester
The Covid-19 pandemic and the measures taken (from March 2020 to early January of this year) to prevent and manage its spread in the prison environment, played additional roles in further alienating prisoners from the already limited activities which aim to contribute to their rehabilitation. It stands to reason, that an absence/suspension of these activities and programs (for approximately two years) as well as the pandemic itself, likely intensified feelings of stress and depression amongst prisoners. Prison staff who too were subjected to strict Covid-19 guidelines including prolonged periods of confinement in the prison environment likely experienced increased levels of stress on their mental well-being.
Among the measures taken was the suspension of all religious activities and training programs within the prison. One of the key findings unearthed during the interviews conducted in 2019, revealed that religion is one of the biggest coping mechanisms utilized by prisoners, as attending religious services gives them comfort and relieves feelings of stress, depression and hopelessness. These findings are not unique to Guyana’s prison environment, as several studies conducted in other jurisdictions point to the effectiveness of religion in positively impacting the mental health of prisoners. Bradshaw and Ellison 2010, and Ellison et al, 2008 for instance, note that “Participation in religious activities can impact inmate mental health by promoting social support. Attendance at religious services has consistently been shown to be protective against mental distress.”
The suspension of this vital stress-reliever and depression-combatant implies that many prisoners were likely to become withdrawn, easily agitated, disruptive, fight amongst themselves, experience appetite loss, and harbour escape and/or suicidal thoughts.
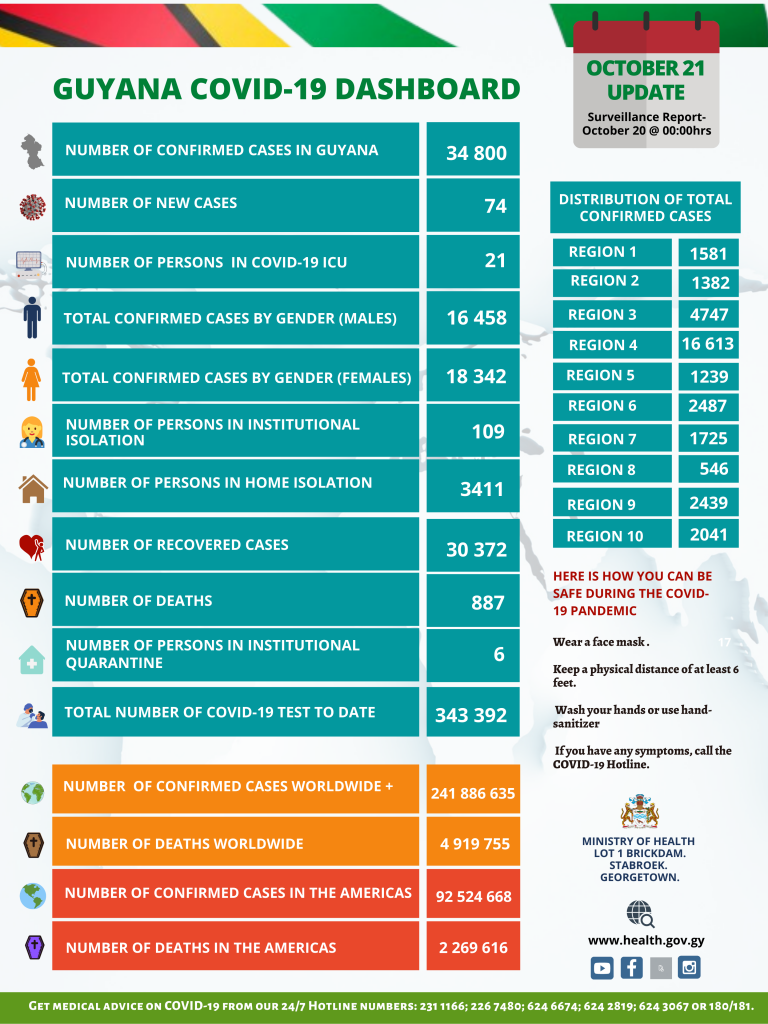
Given that the number of daily Covid-19 positive cases, both outside of and inside of the prison contexts of Guyana has drastically reduced from its peak of 1,558 on January 17 of this year to 5 cases as at March 25, 2022 (WHO), and also given that there is already inadequate mental help support in the form of counselling and therapy for convicted prisoners and that no such service exists for prisoners on remand, it is recommended that religious activities should be resumed, albeit in the contexts of social-distancing, sanitizing and mask-wearing guidelines. Conscious of the limited spacing available for religious worship due to massive overcrowding, small groups could be accommodated at various intervals in order to fulfil the right of prisoners to religious engagements which is vital to prisoners’ mental well-being as well as their rehabilitation.
With respect to training activities, those too were suspended for approximately two-years. However, between January 12 and 15 of this year, all of the Guyana dailies and Newscasts reported that 861 prisoners housed at the various prisons graduated in what is being referred to as “ground-breaking” training courses offered at the various prisons. The programs, prison officials’ note, aim to prepare inmates for life outside of the prison and to assist with their reintegration into society. The inmates had the opportunity to participate in a number of different training areas such as entrepreneurship, anger management, carpentry and joinery, family reconciliation, tailoring, culinary arts, art and craft, cosmetology, barbering, crops husbandry and veterinary sciences. The courses were extended to all prisoners including those on remand and also those who were convicted with several high-profile and special watch inmates taking the opportunity to rehabilitate themselves with the courses. (HGP Nightly News. January 15, 2022). Further, the “Fresh-start” program launched just last month by the Guyana Prison Service with similar programs and more, are all aimed at preparing prisoners for productive life outside of prison. (Stabroek News. February 18, 2022)
These programs must be commended for their role in fostering prisoners’ rehabilitation and likely reducing rates of recidivism as “the impact of education goes well beyond the walls of the prisons themselves, extending into the home communities of the incarcerated.” (North Western University Prison Education Program). Their importance in assisting the mental health of prisoners whose time would have been more than likely spent on unproductive activities which contribute to depression, anxiety, stress and other mental ailments cannot be overstated. Further, the inclusion of these programs to prisoners on remand must also be applauded for its progressiveness given that the current laws do not extend those privileges to remand prisoners, many of whom sometimes spend several idle years behind bars before sentencing or release.
Another of the measures taken was the suspension of the (external) work rehabilitation program. Prior to the pandemic, some prisoners were able to capitalize on work rehabilitation programs which not only helped in the provision of financial resources for them to supplement their prison-provided supplies, but also contributed to their families’ upkeep, occupied their time, helped provide meaning in their lives by providing them with something to focus on, and prepared them for post-prison productive life. North Western University Prison Education Program notes that work rehabilitation aids in preparing prisoners for life outside of prison as “reentry is far smoother and more successful for those who took classes in prison, especially insofar as gainful employment is one of the defining features of successful reentry.” The suspension of this privilege likely impacted the mental health of prisoners in a negative way. Existing literature suggests that “inmate boredom caused by the lack of work and absence of recreational activities could be linked to depression and aggressive behavior.” (Tartoro and Leaster, 2009). Such behaviors could spread among the prison population thereby leading to prison riots, fires etc., all of which could make the work more challenging for an already thinly-stretched and over-worked prison staff.
The suspension of family visits was another measure implemented to prevent and manage the Covid-19 pandemic in Guyana’s prison setting. During the interview sessions with prisoners in 2019, many bemoaned the lack of/limited visits form their family members, while others were in praise for supportive family members who visit often and supplement their supplies. The complete removal of this social support privilege (though replaced by electronic means using the “Google Hangouts app” and/or telephone) likely increased feelings of depression and other mental health issues amongst prisoners. De. Claire Dixon, 2015 notes that “Visits help offenders to maintain contact with the outside world, promoting successful reintegration back into society and reducing recidivism. This scarcity of social support might make adjustment to prison more difficult, risking the use of maladaptive coping strategies.”
A further measure taken was the suspension of actual (face-to-face) court hearings, and the establishment of virtual courtrooms. While this measure must be lauded for its role in respecting the rights of prisoners to a trial within a reasonable time period as well as the possible reduction of time spent on remand, the positive mental-health benefits of actually leaving the confines of the prison environment for a trip (however temporary), to be in a setting with non-prisoners, to perhaps have a moment to socially interact with family members and their attorney, cannot be ignored.
While most of these measures impacted prisoners, their impact on the mental-health of prison staff cannot be ignored. Prison Officers were already in-line due to the prolonged March 2020 elections and they were forced to remain in-line (for time frames as long as two weeks) as a precaution against bringing the virus into the prison environment. Devoid of the vital social interaction of family, being forced to work long hours in an overcrowded setting in the face of a massive human resource deficit, fearful of contracting a deadly virus in the contexts of agitated, violent, dangerous and scared prisoners are all factors which likely intensified the stress levels of prison staff.
It should be recalled that a number of undiagnosed prisoners, specifically those on remand, complained of experiencing bouts of depression and anxiety as a result of their incarceration. They also bemoaned the absence of competent mental health personnel on whom they could unburden themselves. Similar sentiments were expressed by officers and other prison staff who, like most prisoners, also use religion as a coping mechanism.
In light of the foregoing, and in the context of the almost- completed “modern” prison and proposed new prison headquarters at Lusignan, it is hoped that this facility would be equipped with a modern mental health facility and staffed by competent metal-health personnel, including therapists and counselors to assist prisoners (including remand prisoners who do not benefit from existing arrangements) and prison staff.
Such facility would greatly augment prisoners’ rehabilitation, prepare them for life outside of prison and ultimately reduce the rates of recidivism. For Prisons Officers and other staff, working in both one-on-one and group sessions with a therapist could help them cope with the challenges associated with a highly stressful, time-consuming, low-paying, and sometimes under-valued profession.
By Clare Anderson, Mellissa Ifill, Remi Anderson & Shammane Joseph-Jackson.
All over the world, the COVID-19 pandemic has impacted on prisons, particularly where institutions are overcrowded. In Guyana, where prison capacity hovers at around 125%, until 15 September 2020, no prisoners were known to have had the virus, but on that day two prisoners at Lusignan Holding Bay tested positive. COVID-19 quickly spread in the prison, and by the end of the month 218 inmates had returned positive tests. To date, the overwhelming majority of infections in the prison system are in this location (around 70%). This is due to the fact that Lusignan is the main prison for new admissions, which accounts for the majority of new cases. The others were mainly split between Timehri and Mazaruni, with smaller numbers in New Amsterdam and Georgetown (Camp Street). Up to now, October 2021, one prisoner has died at Mazaruni, though following the Lusignan infections a hunger strike and attempted outbreak led to the death of two inmates who were shot dead whilst trying to escape.
In the current pandemic, Guyana’s prisons have attracted even less than normal attention and resources. With the exception of public statements by the Guyana Human Rights Association, civil society has largely been unresponsive to the plight of prisoners in COVID-19. It has recommended that all sentences for possession of marijuana or other secondary category drugs be commuted to time served, all remand prisoners for non-violent crimes be reviewed and bail reduced, all prisoners whose sentences are within three months of completion be released early, and all women prisoners for non-violent offences be commuted.
Pandemic prison guidelines were initially developed from the more general guidelines issued by the Ministry of Public Health and National COVID-19 Task Force, and also influenced by best practices yielded from the 2020 International Conference for Prison Services in Latin America and the Caribbean. Guidelines included the establishment of isolation and quarantine areas, early release of some inmates, setting up of virtual courts, suspension of prison visits, new staff work schedules (14 days on/ 14 days off, to reduce ingress and egress), and new sanitation and cleaning practices. Since last autumn, these were augmented with the mandatory use of facemasks for inmates and staff, testing of new admissions, and the provision of buses for staff – to mitigate the risk of infection while travelling to and from work. Staff are briefed in daily meetings, with frontline officers required to oversee daily operations, ensuring that safety measures are adhered to or alternative arrangements put in place.
The safety measures seem to have worked well within the institutional, systemic, resource and infrastructural constraints of the prison system. There has been a reduction in the inmate population, the result of close collaboration between the judiciary and the prison system, and the more routine use of bail and community service sentencing. However, there is no question too that the pandemic has exacerbated chronic staff shortages, including through fear and concerns about safety. The remoteness of some sites, such as Mazaruni prison, has further added to these concerns as vaccination rates among staff remain significantly lower than elsewhere in the service. Staff absenteeism led to increased incidences of agitation among inmates, and complaints and demands to see the welfare and medical officers. Prisoner concerns included lost opportunities to work and earn; remission of sentences; loss of family visits; inability of some families to take advantage of virtual visits; and poor internet capacity which interrupted virtual visits with attorneys and families and caused trials to be rescheduled.
Prisons present ideal conditions for viral transmission, and the prevention of social contact in them has been a priority in numerous global locations. Overall, the cautious and pragmatic approach of the Guyana Prison Service during the early months of the pandemic impacted on prisoners’ access to justice and rehabilitation, and increased tensions inside the jails. Moreover, though there have been attempts to limit it, the ingress and egress of staff and supplies means that it is not possible altogether to eliminate the entry of the virus into prisons.
Later on, digital technologies enabled the resumption of trials and visitations. However, these digital strategies, while useful and reportedly spurring the courts on to increased productivity, have removed the human centred approach in circumstances where prisoners and their families are not entirely familiar – or even familiar at all – with new technological innovations. It is important therefore, that care is taken not to perpetuate inadvertent discrimination in such contexts. And, as Guyana rolls out its vaccination programme the cost of this is in terms of enhancing inequalities for some sectors of the population remains to be seen. Important questions for the future also remain. Will the measures instigated over the past year remain effective? And what will be the long-term impact of the pandemic on the health and mental well-being of staff and inmates?
This research was a collaboration between the University of Leicester and University of Guyana, in partnership with the Guyana Prison Service. It was funded by the University of Leicester’s QR Global Challenges Research Fund (Research England) and led by Professor Clare Anderson.
On 2 March 2016, unrest broke out in Guyana’s oldest and largest prison, Camp Street in Georgetown. Prisoners set fires, leading to the death of seventeen inmates and the partial destruction of the facility. The day after order was restored, President David A. Granger ordered the establishment of a Commission of Inquiry. Inmates had released video footage from inside the prison, blaming individual officers for events, and alleging that they had been locked in their cells and left to die. Granger thus directed the Commission to report on the ‘causes, circumstances, and conditions’ of events, to establish the nature of the prisoners’ injuries, to assess whether the staff of the Guyana Prison Service had followed correct procedure, and to determine whether the inmates’ deaths were caused by the ‘negligence, abandonment of duty, disregard of instructions, [or] inaction of the Prison Officers’. He also ordered it to make recommendations necessary to secure the future safety of the prison.
The commissioners undertook an expansive investigation, visiting the prison and interviewing numerous witnesses. They concluded that ultimately inmates themselves were responsible for the deaths, because in the intense heat prison officers had been unable to open cell doors. However, they also laid the blame on ‘a myriad of institutional deficiencies’ that were products of Guyana’s punitive attitude to crime and public apathy about prison conditions. The Commission described the huge backlog of court cases, which meant that at the time of the fire two thirds of inmates in Camp Street were on remand, with the prison at 184 per cent capacity. It noted that these delays were in part a consequence of the courts’ under-use of defendants’ constitutional right to bail, but that overcrowding generally was also the result of harsh sentencing policy, including for relatively minor drugs-related offences. Further, the Commission blamed the system of preliminary inquiries, the lengthy pre-trial process of gathering oral evidence, which slowed the progress of cases through the courts.
Cover page of the 2016 Camp Street Commission
Its recommendations for the Guyana Prison Service included enhanced training for officers, greater attention to inmate welfare, and the development of infrastructure. For the judiciary and magistracy, it advised more routine granting of bail, and the abolition of minimum sentences, the decriminalisation of cannabis for personal use, alternatives to custody for petty drugs-related offences, and greater attention to proportionality in sentencing. Finally, it highlighted the desirability of a publicity campaign to address punitive attitudes and educate the public about the importance of rehabilitation.
The 2016 Commission of Inquiry was by no means the first investigation into prisons in Guyana. Indeed, such commissions have a long history, and date from the British colonial era. Commissions were appointed and instructed by the governor, and they had the right to call witnesses and take evidence on oath. Commissioners reported to the legislative council, which discussed their findings and could pass resolutions. Following Independence in 1966, this practice (as codified in a 1933 Act) was incorporated into Guyana’s constitution. Whereas during the British period, the governor was responsible for instigating enquiries, after 1966 this power became the gift of the nation’s president. There are other procedural continuities between the colonial and modern periods. Then as now, commissions are independent of government, and charged with establishing and regulating their own procedures. Whilst previously the British announced commissions in a special supplement of colony’s official newspaper, TheRoyal Gazette, today they appear in Guyana’s The Official Gazette.
The first prison commission that I have been able to locate in the archives took place in 1847. It was focused on Mazaruni, as were the majority of the inquiries of the colonial period – a 1906 inquiry into Georgetown is the key exception. This was probably due to Mazaruni’s remote location, which at the time was seen as the cause of the allegations of violence, cruelty and corruption that surfaced periodically. Since Independence there have been further commissions, again centred on Mazaruni and Georgetown, but also on New Amsterdam and Lusignan. In sum, I have found evidence that there have been a dozen commissions into prisons since 1847. Given the fragmented nature of the archives (not all documents survive) there may have been more.
Together, these inquiries – including interviews with British and Guyanese personnel, and inmates – tell us quite a lot about ideas about punishment and rehabilitation. Where commissions published summaries of interviews with prisoners and front-line personnel, they also enable rare glimpses of the experiences of ordinary Guyanese, and in particular of the nature of everyday life in jail. Witness statements were taken formally and verbally. During the colonial era, where an individual was the subject of an inquiry (e.g., when a British officer was accused of violence), they were present at cross-examinations and allowed to ask questions. Though in law inquiries were not judicial trials, they certainly mirrored their form.
Reading archives of prison inquiries against our knowledge of present-day practice leads us to ask certain questions. Historically, were commissions an effective tool of governance? To what extent did they address crisis and controversy, rather than structural or deep-seated issues? Did they legitimize state authority and maintain colonial interests rather than push for change? To help to think these issues through, let us explore some historic examples.
The 1847 commission that I mentioned above was set up to investigate an alleged plot by inmates to murder the superintendent, poison the guards, and set fire to the buildings, against a background of widespread social unrest following a dramatic drop in wages in the years after emancipation. The Commission did not contextualise events at Mazaruni, or connect the colony’s jail building programme to the end of enslavement, but instead resolved only to open negotiations on the establishment of a military post nearby, to enhance security.
A second inquiry of 1848, again at Mazaruni, was ordered in the aftermath of the deaths of twelve inmates, due to the violence and neglect of the medical officer. He fled, and though the inquiry took evidence, and a warrant was issued for his arrest, the legal process against him could not begin in his absence, and there were no changes to prison management as a consequence. These were put in place only in 1854 and 1855, following the removal of a second medical officer from Mazaruni, for frequent drunkenness. The most important stimulus to change here, however, was not the inquiry itself, but simultaneous Colonial Office pressure on the colony to bring jail rules and regulations into line with those in place in Britain. (That did not happen, though there were some minor alterations).
Printed for the Colonial Office – the 1872 report
The biggest changes came in the 1870s, when a request was sent to the governor, asking for a change in practice in medical postings at Mazaruni, alongside extensive details of the prior history of the site. The issue was referred to the colonial secretary, the 1st Earl of Kimberley, and referring to previous ‘abuses and cruelties’, he expressed regret that Mazaruni was still open. A new commission was set up, and this made various recommendations about the rotation of officers and the building of better officer accommodation. Backed by London, these were put into force. If the picture of change and continuity is somewhat variegated in the colonial past, how about the outcomes of prison commissions since Independence, and particularly that of 2016?
Almost five years on, the Commission does seem to have catalysed the construction of new accommodation at Camp Street, as well as at Mazaruni, though neither is yet open. Work on better officer training is underway, and there has been a little movement in regard to issues such as the granting of bail or the abolition of minimum sentences, particularly to address overcrowding in light of the Covid-19 pandemic. The country is now also experimenting with the use of a separate Drug Treatment Court. Until the new facilities are open, however, the Guyana Prison Service cannot properly address the key issue highlighted by the Commission: overcrowding. Bodies such as the Inter-American Development Bank are now working towards a reduction in the prison population across the Caribbean. Whether these initiatives are enough to reduce punitive public attitudes remains to be seen. Certainly, evidence-based research, such as that generated through the MNS Guyana project, can only assist in that endeavour.
Author’s acknowledgement: Thanks to Kellie Moss for photographing the 1872 report, and Mellissa Ifill for comments on an earlier draft.
I never had cause to visit a prison. In fact, my only experience with the penal system was through visits to a nearby police station to take a meal for, or to offer support to a friend or relative detained for some minor infraction which did not require lengthy incarceration.
This situation changed for me when I became involved as Research Assistant on a University of Leicester-University of Guyana research project titled “MNS disorders in Guyana’s jails, 1825 to the present day,” which seeks to determine the definition, extent, experience and treatment of mental, neurological and substance abuse (MNS) disorders in Guyana’s jails: both among inmates and the people who work with them.
This blog offers a glimpse of my journey into prison research and the impact of this journey on my own personal awareness of the problems of incarceration.
A UK-based colleague with Trinidadian roots, Dr. Dylan Kerrigan and I were tasked with conducting interviews with prisoners housed at the Georgetown (Camp Street) and the Lusignan Prisons, in which a number of themes were explored including area/s of residency prior to incarceration, family life, education, childhood experiences, employment, reason for incarceration, experiences in prison life, hope for the future and so on. Twenty such interviews were conducted between the two prisons and included respondents that were clinically diagnosed with a MNS disorder and others who were not.
Prison security is “tight.” Once the reason for your visit is ascertained and accepted, everyone is then searched for prohibited substances and articles. I observed, how diligently and professionally the officers carried out this function. I recall observing a staff attached to an external janitorial company being refused further access to the facility after he refused to have his footwear searched. We were also required to lodge our handbag and backpack along with their contents (cell phones, money etc.) at the security hut; only writing materials, a voice recorder and other requisite paperwork were we allowed to take to the interviews.
Lusignan Prison was built after independence, on the grounds and land of a former plantation hospital that today is also a current landfill and rubbish dump. The prison compound is however well-kept. One of the prisoners interviewed took credit for the well put-together flower garden located at the front of the prison. Most of the buildings are wooden structures; old and dilapidated and in dire need of repairs if not complete demolition.
Photograph of Lusignan Prison Walls, by Professor Martin Halliwell, University of Leicester.
One of the things that struck me on my first day at the Lusignan Prison was its tranquility. There was a hum, but it was heard only when you actually focused on it. I think I was expecting that a facility in which hundreds of men are housed to be noisier; with chatter or laughter, or arguments. Prisoners in the prison yard also moved about quietly and purposefully and were always polite to us.
By day three, word must have gotten around about the nature of our research. On our way to the Chapel they (prisoners) would call out to us, some would request to be interviewed, some perhaps just happy to see two different faces which were becoming familiar to them.
The prison Welfare Officer was the personnel at Lusignan who organized and supervised our interviews with the prisoners. She was professional and courteous, and also happened to be a former student of mine. She would escort us to the Chapel which is almost always occupied with prisoners who had just concluded church services. The worshippers were always eager to assist with setting up the seating arrangements to our satisfaction and comfort.
Most of the prisoners, except for perhaps one, volunteered to be interviewed. We sought to understand the history and background of the prisoners; specifically, information which related to their early life; family, neighbourhood, education and employment. We also sought to ascertain the reason for their detention/incarceration, how they cope with prison life, their history of substance use and/or abuse both outside of and in prison, their mental health, views of themselves and society and their plans after release. The data obtained from the interviews was in some ways predictable, but it was also surprising, intriguing, shocking, and encouraging to me as a free individual.
Predictably, most of the prisoners interviewed were Afro Guyanese and followed sharply by Indo Guyanese. Mixed-race respondents followed and there was a tiny percentage that was indigenous Guyanese. The majority came from economically and socially depressed communities in Georgetown. There was also one Indigenous respondent who hailed all the way from Lethem, Region 9.
In addition to their community of origin, many of the prisoners came from families of predominantly single-parent households with absent fathers in most instances, and many siblings. In several cases, children were raised by grandparents and or other relatives when parents were either working away from home, or in the event of death of the parents, or due to their parents’ inability to provide for them. Additionally, most of those interviewed were school drop-outs, some at the primary and others at the secondary level. Many never wrote or got the chance to write the Caribbean Examination Council (CXC) examinations and thus lacked the basic requirements for clerical employment and higher education. Many sought unskilled work in areas such as in construction, others became mini bus conductors and peddlers in order to assist the family. Some started selling and/or using drugs; predominantly marijuana, while some got into trouble with the law after getting involved in crimes such as robbery; theft of phones, handbags break-and-enter etc. These socio-economic findings are regarded as “predictable” because the literature is replete with similar findings in the context of developed as well as developing countries.
Despite these, there was at least one prisoner who grew up in a financially well-off nuclear family in an economically vibrant community and is highly educated in the medical field. There was also one who studied at an overseas university for a while before quitting and one who is an educated sports umpire.
The vast majority of prisoners we spoke with were at the time on remand and were awaiting trial. The reasons for prisoners’ incarceration were many, but the charges of murder, manslaughter and assault stood out. A few of the murders were allegedly committed while drunk or high on narcotics, and a similar pattern was observed with the assault-related offenses. One (educated) prisoner decried the fact that he was sentenced for physically assaulting his wife while drunk. For him, it was a personal issue, and should have been dealt with in the domain of the home. (I still hope that the shock I felt at that position did not register on my face.) Most felt that being a man meant that they were the dominant partner in relationships (of marriage and the family) and see their role as that of providers. Being a man means acting like a man; tough and masculine. These positions are historical legacies of colonialism with respect to hierarchy, masculinity, gender and gender roles, and remain largely intact even today, both in and out of prison in Guyana.
A small number of prisoners were detained for drug-related offenses and some for robbery and theft. Many (especially murder accused) decried the lengthy time it took for their cases to be heard, and said they were receiving little information regarding their case. The Welfare Officer said that such information is always provided to prisoners.
Life in prison is boring for the vast majority of prisoners. Most argue that they don’t do much per day, passing the time reading (the Bible especially), sleeping or interacting with fellow cell or dorm mates. Some work in the kitchen preparing meals, others in the store, in the prison garden, or on the prison farm, others clean the grounds. At scheduled times, batches of prisoners are allowed to play sports in the prison yard. Cricket is one such games played at Lusignan. The prisoner with umpiring experience told us with pride and happiness, that he umpired some cricket matches which helped to lift his spirit. We also noticed some prisoners exercising in a very basic gym located on the ground floor a few feet away from the Chapel, while others played dominoes. Some prisoners are able to work for wages, outside of prison mostly in the area of construction or on farms. Employment provides them with the opportunity to assist their families financially, and also to provide themselves with additional sanitary and other supplies.
The majority of prisoners we interviewed are highly religious; predominantly Evangelical Christians, and attend church services frequently to pass the time. One respondent said he practices Hinduism on the outside, but would attend church services at times to help him cope with the stress of prison. Islam is also practiced at the Lusignan Prisons, and a separate space is provided for this purpose. Religion thus appeared to be one of if not the best coping mechanisms utilized by most prisoners. Almost every interviewed prisoner said that they are trusting God for his favour in terms of early trial, early release, light sentencing or even dismissal of their case. Even those against whom evidence seems stacked high remain optimistic that God will see them through. Apart from being an excellent coping mechanism, religious practice carries incentives to prisoners as attending religious services coupled with good behaviour aid in sentence commutation which translates to early release. Prisoners are not the only ones who lean on religion to cope. Some prison staff whom we spoke with informally also relied heavily on religion to help them deal with the pressures of work in the prison setting. One prison staff remarked that she talks to, and relies on her Jesus for strength in times of stress as there is no institutional mental health support for staff.
For most prisoners interviewed, cigarettes and marijuana have also been regarded as excellent items which aid in making life easier for prisoners. As a matter of fact, many said that they used either or both substances prior to incarceration. Prisoners including orderlies said that these two items have a calming effect on prisoners as they tend to sleep or lie quietly in their cell after using said items. This makes the job easier especially for prison officers as conflicts amongst prisoners (which require greater supervision) are drastically reduced. I suspect that this is perhaps one reason why prison officers turn a blind eye to marijuana smuggling and cigarette and use in prison although marijuana is an illegal and prohibited drug.
Most prisoners said that they have never witnessed the presence, or use of crack or cocaine in prison. It is almost the same for alcohol, although media coverage highlighted this in the past. A few of the prisoners interviewed were alcohol users or perhaps abusers prior to incarceration. In fact, some are in prison because of violent inter-personal crimes committed while intoxicated. Though alcohol is not popular in prison, there have been instances of prisoners making home-made or prison-made wine called “kushung peng,” also a prohibited substance. This wine is made from the skin of fruits and vegetables which are soaked for approximately two weeks. One Prison Officer in an informal conversation noted that the making of this wine is prohibited especially because of its effect (temporary) on the behavior of some prisoners. Some of the prisoners’ exhibit violent behavior towards other prisoners, some become psychotic; claiming to see spirits or hear voices, while some become loud and disruptive. These behaviours make the work of prison officials more challenging.
Some of the prisoners (approximately half) interviewed were clinically diagnosed with a mental health condition. These conditions include depression, psychosis, schizophrenia, multiple personality disorder, stress, compulsive lying and anxiety. One claimed to be a lion, and roared a few times for us. Another said he laughs out loudly at times, and because of this, persons seem to think that he is crazy. Some prisoners bang their heads against the cell walls while others almost never speak to anyone. At least one prisoner reported that one of his deceased parents had mental health condition, a trait he might have inherited. All of the prisoners interviewed complained of feeling depressed regularly. There was one prisoner that exhibited symptoms of multiple personality disorder who claimed to have been physically abused by his father for displaying “girly” (feminine) behavior and entered a life of petty crime to prove his masculinity. This trauma perhaps contributed largely to his illness and might be responsible for his incarceration.
Most of the clinically diagnosed prisoners are housed in the “Chalet” (a space in prison dedicated to inmates with mental health condition/s) of the prison. All of these prisoners are patients of Guyana’s renowned psychiatrist Dr. Bhiro Harry who makes frequent scheduled visits to the Chalet. Tables are given to some inmates, while injections are administered to others. Some complain that the medications (especially the injection) have a negative effective on them, causing them to drool and feel lethargic. Others complain that the tablets make them sleep a lot. There was one inmate who praised Dr. Harry for finding the correct medication and dosage for his many mental health conditions, and plan to continue in the doctor’s clinic when released. Of note is the fact that some of the diagnosed prisoners denied having a mental health condition. This could be attributed to the historical and continuing stigma attached to mental illness in Guyana, ignorance, or perhaps shame.
Some of these prisoners claimed to have experienced para normal activities in prison. Some said they have seen evil spirits and heard footsteps that turn out to be no one. One prisoner said that he was constantly tormented by a renowned ghost at the Mazaruni Prison. He said he begged to be transferred because of this, but continued to have the same experience at the Lusignan facility. Others claimed to have had sexual encounters with the beautiful spirits in their dreams who leave them “hanging.” There was one prisoner who suffers from epilepsy, and thinks that his condition could be helped if he gets to visit Suriname for “spiritual” healing because for him, his condition is not medical/neurological.
A small percentage of the prisoners said that they participated in the Anger Management Program. This program appears to combine religious teachings in its curriculum/application and is lauded by those who participated in it as a good initiative which aids in self-control.
Most of Guyana’s prisons seem to be overcrowded. This was exacerbated by the 2017 fire at the Georgetown Prison which destroyed several buildings including dormitories and cells, and resulted in the transfer of hundreds of prisoners to Lusignan. Some prisoners are therefore forced to live in cramped cells, at times having to share a single-mattress with another cell mate. One prisoner bemoaned the fact that some are forced to sleep in very close proximity to the toilet facility which is both unhealthy and inhumane. Concerns were also expressed about the lack of privacy one has when answering to calls of nature or taking a shower as the bathroom stalls are not equipped with doors or curtains. Food complaints were few, though at least one prisoner complained of needing larger portions.
Most prisoners regard many of the Prison Officers as “alright” or good people who don’t mistreat them. Violence towards prisoners by Prison Officers appear to be rare, and is utilized against prisoners who are extremely disruptive or violent towards each other. Similarly, the prisoners noted that there are not much prisoner to prisoner violence in the prison itself. Many of the news stories of violence and death at the Lusignan facility tend to take place in the holding bay; a make-shift facility erected at the back of the compound to house prisoners on remand.
For some prisoners, more televisions along with sports channels would make prison life a bit more bearable. The need to greater access to marijuana and cigarette to a lesser extent, seem to be the biggest desire for prisoners’ comfort. Marijuana is an illegal substance in Guyana which carries a maximum sentence of three years in prison. Despite this, most prisoners made it clear that they shall not stop its use in or out of prison.
Many miss their families and long to be reunited with them. For some, their relationship with family (especially their spouses) has suffered as a result of their prolonged detention. Some expressed their gratitude for the visits and material support offered by family members, a few lamented the lack of care and compassion given the absence of visits or any other form of support from family members, while at least one prefers that his family members not visit him at the facility in the interest of their safety.
Many prisoners seem optimistic that they’d be released from prison soon. Most place their faith and trust in God realize this dream even when the evidence seems stacked against them. While most claim to be innocent of all charges, there were a few who admitted culpability for their actions and pledged to lead a more productive and law-abiding post-prison life.
Life outside of prison might prove challenging for a few prisoners who claimed to be homeless with relatives unable but more so unwilling to house them, even temporarily. At least one prisoner expressed the need for temporary housing for former prisoners until they get back on their feet.
The position of one man accused of murder whom I recognized form being on the news, and who claimed to not recall the reason for his incarceration intrigued me. He said he does not wish to be released from prison; that he prefers to remain incarcerated. We tried to determine why this was so, but he refused to provide us with a response. I think that the combination of shame for his actions and fear of retribution by the family and community of his victim have made prison a safer place for him.
We sought some advice from prisoners before we concluded most of our interviews with them. The resounding advice revolved around the need for us to stay out of trouble to avoid incarceration; an advice well received.
The experience with prison interviews and prisoners have left lasting impressions on me as a free individual. I have a new-found respect for the capacity of humans to be resilient in the face of insurmountable challenges. Being confined in a small space with complete strangers for a prolonged period of time is enough to send one over the edge, but most prisoners cope; they remain optimistic about their future thanks largely to another colonial legacy – Christianity. The simple things that bring them happiness; marijuana and cigarettes, are things sometimes frowned upon by free peoples or may be prohibited by law. Policy makers need to revisit such laws, for I am convinced that prohibition or incarceration will not stop marijuana use.
The value of freedom is ever present in my consciousness and I often find myself utilizing the experience I’ve gained and the lessons I’ve learned during those prison interviews to caution as well as counsel many young men in my community. I trust that my words of counsel bear fruit.
The ‘Penal System’ is said to have two functions: the protection of society and rehabilitation. These are set out to sometimes be at odds and also both undermined by similar forces.
Guyana Prison Service Training Unit 1974
Last October, during an event held to mark Guyana Prison Service (GPS) week, Director of Prisons Gladwin Samuels addressed the importance of prisoner rehabilitation. He said that the punitive measures favoured by many do not help to increase security in the long term. Rather, Samuels explained, rehabilitation benefited not only prisoners but was also necessary for the security of individuals and society.
Samuel’s vision of rehabilitation includes academic and vocational training, alongside programmes for addressing the psychological and social needs of prisoners. The attempt to facilitate a robust rehabilitation programme faces a number of barriers within prison. This includes a lack of funding for rehabilitation programmes, issues of attracting and retaining qualified educators and trainers, overcrowding and a lack infrastructure suitable for such programmes. Some of these issues have existed for a very long time but have been exasperated in more recent years. This is in part because of fires which destroyed parts of two facilities over the past four years which led to an even further reduction of space available for holding prisoners. As a result, cafeterias and training areas have been turned into cells in a number of the facilities.
The long term success of rehabilitation programmes is challenged by what ex-prisoners face once released from prison. For stigma against ex-prisoners remains along with decreased employment opportunities. Some former prisoners also face a lack of sustained support from family and friends.
The present goals for rehabilitating prisoners and the barriers faced echoes issues faced by GPS in the 1970s. In the summer of 1974 the ‘Crime and the Penal System in Guyana’ conference was hosted by the University of Guyana. This was the first such conference held in Guyana and the second in the ‘Caribbean region.’ It brought together researchers and practitioners to explore studies concerning crime as well as the experience had on the ground by those working in the criminal justice system and prisons. The aim was to create a ‘cooperative approach’ among the various ‘branches of the criminal justice system’ in Guyana in order to better face the issue of crime in society.
At this conference Edwin Pratt presented a ‘Report on the Operation of the Guyana Prison Service’ which had been prepared by the staff of the GPS Training Unit. The report began by outlining what they felt was the purpose of the ‘penal system’ which is outlined in the quote at the beginning of this blog. The report explains that the tension between rehabilitation and security is in part due to prison infrastructure. For maximum security prisons were set up to keep prisoners inside and did not have the facilities needed for the ‘meaningful rehabilitation of inmates.’ It explained that a certain amount of freedom was needed in order to bring about true rehabilitation which was in conflict with the aim of maintaining maximum security. Furthermore, a lack of finances meant that there not enough money to run an effective rehabilitation programme or maintain security. The report called on the government to make ‘the penal system’ more of a ‘priority.’
Later on in the report is a description of prisoners as a ‘section of the nation’s human resources.’ The way in which prisoners are described here gives some indication of an inclusive idea of citizenship in which all members of society should contribute to the nation. These ideas, at least in part, stretched to approaches to the treatment of those who had been convicted of crimes and imprisoned. This focus on the nation, which was less than a decade old, was also found in the desire to use ‘modern’ methods of rehabilitation as opposed to colonial forms. Interestingly, these new forms were in part learnt from prison officials in Britain, Guyana’s former coloniser. And while these methods offered a shift away from what had come before, they did not provide a comprehensive critique or alternatives to the use of prison for the punishment and reform of those convicted of crimes.
And yet, the focus on modern forms of rehabilitation did require a new way of thinking among prison officers. In the report, ‘a purely punitive traditional philosophy’ is set in contrast to ‘the modern concept with its emphasis on the rehabilitation of the inmates.’ The emphasis on incorporating ‘modern techniques of rehabilitation’ was thus said to necessitate the recruitment of ‘suitably qualified and interested persons.’ This call for improvement can thus be seen as being part of a process that had already begun. For example, some changes were said to have already been made with regards to the ‘promotion to the rank of Principal Officer and above.’
How was rehabilitation conceived in the 1970s? It involved ensuring the physical and mental health of prisoners, instilling a firm work ethic, providing religious support, giving individuals the chance to gain vocational and academic training, and providing opportunities to play games and participate in sports and the arts. These programmes were seen as being important for keeping prisoners busy while in prison as well as teaching them new skills and habits to prepare them for life after prison. In this we can see both change and continuity within the system of rehabilitation that had come before. Critically, the historic focus on labour continued as the majority of most prisoners’ days were spent working.
Vocational training was ideally meant to form a part of this labour. The report explains that attempts were made to align work assignments with prisoners’ ‘interest, abilities, training needs and trustworthiness.’ However, a lack of training facilities meant that this alignment was not possible with ‘training in the various trades [being] incidental rather than deliberate.’ Also noted was an emphasis on ‘production at the expense of positive training.’ So both an absence of training and a focus on production meant that many prisoners did not receive skills training that would assist them after they left prison.
As evidence of this focus on labour, the report explained that at New Amsterdam and Mazaruni prisons most inmates were employed in agriculture, even though the majority were from urban areas and not interested in agriculture because they would not be returning to a place where they could use these skills when their sentences were done. It was suggested that the emphasis of the agricultural programme needed to change in order to ‘bring about [a] change of attitude and emphasis[e] self-sufficiency.’
Another issue that obstructed rehabilitation aims was overcrowding. The numbers of people incarcerated at Georgetown Prison was described as ‘alarming’. The report explained that the prison, which was meant to accommodate 278 people, was ‘housing almost twice the number that it should normally hold.’ Such conditions were linked to ‘social and health problems.’ New Amsterdam was noted as having ‘acute’ overcrowding and Mazaruni, though described as being ‘far from ideal,’ was said to be better than the other two sites as it held 418 men who each had their own cell. The reports explains that the increase in the prison population hadn’t been met with ‘additional physical accommodation.’ The report offered no consideration of the benefit of reducing the number of prisoners who came to jail in the first place.
Despite these challenges, there were attempts to carry out some programmes even when this fell short the ideal. For instance, education aims included teaching reading to illiterate prisoners as well as providing resources to explore the arts and general interests. Yet, in 1974, there hadn’t been a trained teacher ‘for some time’ with the role of teaching those who were illiterate or who had low literacy levels being the responsibility of ‘a non-specialist member of the prison staff.’
Other education aims had more success. Basic arithmetic was taught, while those who were already literate were facilitated in their studies which included assistance in receiving books and taking exams. Prisoners were given wide scope of what they pursued with education not being narrowly fixed to the process of formal education. The report noted that ‘a prisoner is permitted to pursue any area which is educational in the broadest sense in order to stimulate healthy interests and enlarge his mental outlook.’ As well as individual pursuits, prisoners were able to participate in group events that happened after work such as ‘concerts, debates and plays.’
This report shows GPS’ desire to bring about change by instituting ‘modern’ methods of rehabilitation for prisoners in the 1970s. The attempts were made to incorporate new methods of rehabilitation were hindered by a number of factors including: the maximum security nature of prisons, the focus on labour as production, overcrowding, an inadequate number of trained officers and a lack of funding. This period shows that while an attempt was being made to shift away from colonial forms of imprisonment, the legacies of this system remained in the prison infrastructure and punitive approach to prisons and prisoners that many still had.
Although there are several parallels between now and the 1970s there are of course differences as well. All three of these maximum security prisons are still in use, though they have been joined by two other sites at Timehri and Lusignan. Despite this expansion of facilities, overcrowding remains a significant problem. Both the structure of most prison sites and the numbers of those in prison make it difficult to find adequate and suitable space for rehabilitation programmes. Insufficient funding for rehabilitation programmes is also an issue that is yet to be fully addressed.
The 1974 report notes how some saw the protection of society and rehabilitation as being at odds. Yet both the report and Samuels explain that rehabilitation is necessary for the security of society. Most prisoners have a fixed sentence after which they leave prison. Therefore, the question of security depends in part on recognising these men and women as members of society. The stigma faced by ex-prisoners impacts rates of reoffending by keeping many of them on the margins of society. This adds to insecurity in society by creating more rather than less chances of recidivism.
The author would like to thank Mellissa Ifill for her feedback on this blog.
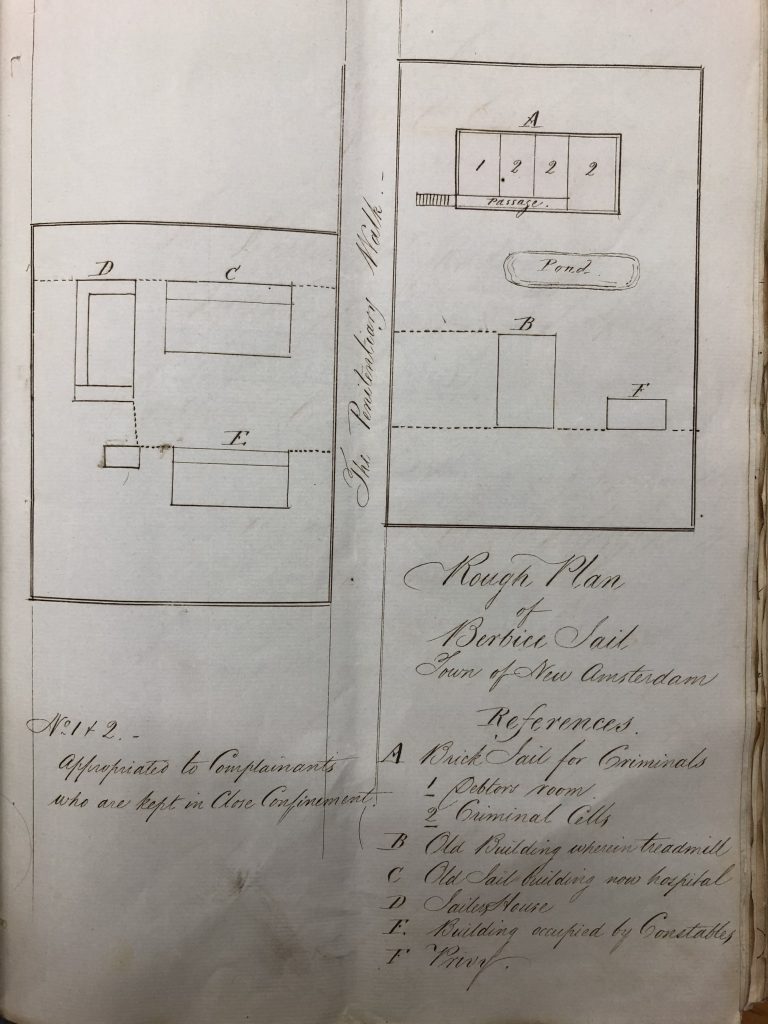
As has become evident as the Covid-19 pandemic extends its grip all over the world today, jails are environments in which infectious diseases can be easily spread. This is especially the case in overcrowded conditions, most especially where prisoners share accommodation and washing and toilet facilities. Historically, outbreaks and epidemics of diarrhoea, dysentery, respiratory illnesses, and whooping cough were the most prevalent diseases in the colony of British Guiana, including in prisons. To these can be added the mosquito-borne illnesses malaria and yellow fever. Limited levels of healthcare and poor sanitation within the prison system meant that after the British began its jail building programme from the 1820s, containing the spread of disease was an ongoing problem. In Her Majesty’s Penal Settlement (HMPS) Mazaruni in 1871, for example, over a third of the prisoners in hospital were suffering from diseases incurred by overcrowding, bad ventilation, and a ‘total lack of any sanitary measures’. The following year, fears were expressed that in the event of an epidemic, Georgetown jail was so overcrowded that the consequences would be disastrous. In fact, this scare underpinned a call for a reduction in the number of prisoners overall, though this did not follow until the first part of the 20th century.
Plan of New Amsterdam Jail, 1841, showing the hospital (“C”)
Despite this recognition, a general lack of concern regarding the welfare of prisoners ensured that epidemics continued to plague the prison system in the decades that followed. Furthermore, once an infectious disease entered the system, the authorities were unable to keep it contained. For example, following an initial case of influenza at HMPS Mazaruni in 1895, recurring outbreaks of the disease were reported in Georgetown, New Amsterdam and Suddie prisons until 1899. The medical officers however, routinely denied any connection between ‘prevalent diseases’ and living conditions. The outbreaks were, instead, attributed to the debilitated condition of the inmates prior to their admittance to prison. This, the medical officers noted, left many prone to catch the disease after only the ‘slightest exposure to chill’. It would be almost 20 years before colonial prison authorities were willing to take responsibility for the conditions that facilitated the spread of infectious diseases.
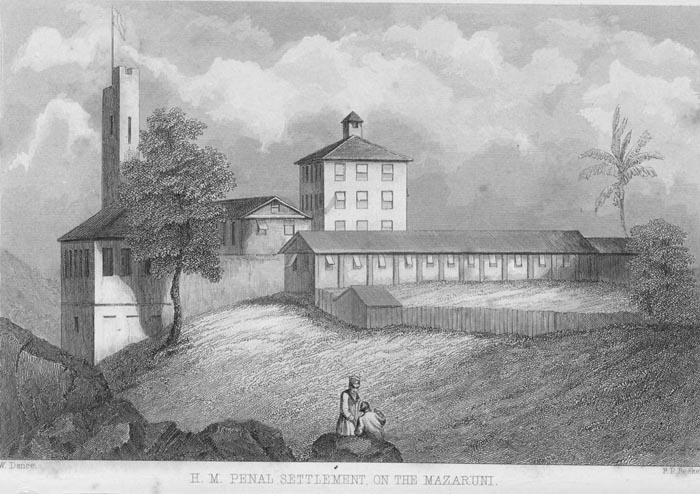
HM Penal Settlement on the Rio Massaruni, c. 1870-1931. Source: The National Archives UK CO1069/355 ‘This view is taken from the side gallery of the Superintendent’s house. The Prison faces East, towards the river. These Halls … are now the oldest portion, and are built of stone … The Union Jack is hoisted on Sundays and special festivals. The Convicts are fallen in on parade, for muster and search before proceeding to labour after their dinner, and represent about 300 men. The end of the roof of the Commissioners’ House is seen to the right among the trees.’
In September 1919, the Acting Surgeon-General of British Guiana J.H. Conyers submitted his usual annual report to Governor Sir Wilfred Collet. In it, he noted the prevalence of the ‘influenza epidemic’, or what we now commonly refer to as the ‘Spanish flu’. What had started out as a mild strain in August 1918, had by November become a severe epidemic that had penetrated the furthest reaches of the colony, including especially dwellings on the plantations. The hospitals of Georgetown and New Amsterdam were, Conyers reported, ‘sorely tested’. In words that resonate today as the Covid-19 virus challenges health systems all over the world, he concluded that the medical service had only managed the situation through deferring all non-urgent operations and other hospital work. Efforts were also made by the health authorities to isolate patients, and their visitors, to eliminate the possibility of the spread of the infection by acute carriers. We now know that the Spanish flu killed between 25 and 30 million people worldwide. The most devastating pandemic in modern history, it affected the whole of the Caribbean, including the colony of British Guiana. It was estimated at the time that out of a total mortality of 8,887 in the months of December, January and February, influenza was responsible for 6,378 deaths. Historian David Killingray puts the figure even higher, at perhaps as many as 20,000.
The influenza pandemic also impacted on the colony’s prisons. From the first recorded patient in Georgetown jail, in December 1918, a virulent strain of the disease spread rapidly throughout the prison population. The transfer of inmates between prison sites meant that cases of the disease emerged soon after in Mazaruni, New Amsterdam, and Suddie. In comparison to previous years the total number of deaths recorded tripled. In 1917, 17 inmates had died in hospital. In 1918, the figure was 30, or 6.5% of the daily average (i.e. the number of prisoners in jail on any given day, not the total number admitted during the year). Although we do not have details of the cause of all these deaths, the Acting Surgeon-General noted the pandemic was to blame for ‘a considerable part’. It was also noted, at the time, how prompt preventive measures by prison authorities, such as the isolation of those displaying symptoms, and improved sanitary measures helped to prevent an even greater spread within the system. This was a difficult task given that fever and dysentery was rife amongst members of the prison staff. Most significantly, however we have no sources that indicate how prisoners and prison officers – or the population at large – understood and experienced the pandemic. Whatever the case, we do know that the overall mortality from the influenza pandemic in the colony was high, as 17.7% of those who contracted the disease died. This figure rose to 21.1% in the colony’s prisons. This means that although a relatively small number of inmates died, they died in larger numbers than the free population. Furthermore, the colonial authorities used prisoners to dig graves in the colony’s capital of Georgetown.
New Amsterdam Hospital, c. 1950. Source: Government Information Agency, Guyana
In the wake of the outbreak, a concerted effort was made by the prison system to enhance levels of hygiene. From this point a small group of prisoners were designated the task of improving sanitary measures within each prison. Efforts to isolate sick inmates and disinfect their cells were also strictly adhered to, although these attempts were not always successful in impeding the spread. Medical officers were often required to convert association wards into temporary hospital bays due to the number of cases, and the lack of suitable medical facilities. At a senior level further attention was also paid to reducing contaminated water supplies, and the breeding of flies, common sources of dysentery and diarrhoea. Yet, despite these efforts intermittent outbreaks of disease continued to plague the colony, although never again on the scale experienced in 1919. For example, there was a localised epidemic at the end of 1933. This caused higher rates of morbidity and mortality overall across the whole colony, but for reasons which are not entirely clear did not impact on prisons.
World Mental Health Day was first observed on 10 October
1992. At that time, globally, not only was mental illness commonly associated
with social stigma, but it was often unhelpfully and sometimes dangerously
elided with cognitive and developmental disabilities. In 1992, the authors of
the ICD (the International Classification
of Diseases, then just into its tenth edition) and the DSM (the Diagnostic and Statistical Manual of Mental
Disorders, favoured in the United States, then awaiting its fourth edition)
were beginning to understand that mental illness spans a range of multiaxial
conditions that require nuanced clinical diagnoses. Both classification systems
recognized that mental illness has an organic cause but is frequently exacerbated
by environmental pressures.
World Mental Health Day, as it was conceived just over a
quarter of a century ago, has been focused on raising consciousness about
mental health and in ensuring mental illness is treated equally to physical
disease. It has also provided a platform to urge governments to adopt policies
that integrate individuals who have been or are being treated for mental health
conditions into community life, rather than long-term hospitalization in often
inadequate state or county facilities. At a time when Western nations, such as
the United States, are witnessing more than 25% of its citizens being treated
for diagnosable mental health conditions, and when a further 25% are likely to suffer
from depression during the course of their lives, it is hard to know where to
begin to deal with experiences that stem from multiple factors, some biological
and others environmental.
The ICD was adopted in the Caribbean region as the official
diagnostic manual by the Pan American Health Organization prior to the
independence of many of its nation states. But, partly due to the colonial
histories of the region, including a tense relationship with Western medicine, the
topic of mental health has only emerged as a priority across the region in the
last decade. During the 2010s, CARICOM governments and advocacy groups came to realize
that heightened awareness is just part of the solution to what the World Health
Organization (WHO) calls a “global health burden” that requires sustained
funding, a robust healthcare infrastructure, and treatment courses that
integrate drug interventions with person-centred therapy. In Guyana, where there
are only 10 trained psychiatrists (3 of them newly graduated in autumn 2019) and
limited hospital provision for mental health care (centred on Georgetown Public
Hospital), and where mental, neurological and substance abuse disorders are
prevalent among the nation’s prisoner population, this is a difficult task.
A starting point for the Guyanese government has been to
increase funding for the Ministry of Public Health to ensure that its Mental
Health Unit (formed in May 2016) has the physical infrastructure to identify,
document, and consciousness-raise about mental health. Led by Dr Util Richmond-Thomas,
the Mental Health Unit has used capital development funding (the mental health
budget was $105 million Guyanese dollars in each of 2017 and 2018, compared to $17
million GYD in 2016, followed by $43 million GYD in 2019) to better integrate
with social care services, to ensure that it is representative of Guyana’s
rural regions, and to prioritise specific causes, such as the 2019 focus of
World Mental Health Day on “Mental Health Promotion and Suicide Prevention”.
This theme dovetailed with World Suicide Prevention Day, which had its own
dedicated date a month earlier, on 10 September, organized by the International
Association for Suicide Prevention in collaboration with WHO. While Dr Richmond-Thomas
recognizes that only a coordinated effort will reduce the health burden of
suicides in Guyana, numerous conversations during my two visits to Georgetown
in April and September 2019 give me a sense of hope that the national health
narrative is on the turn.
Self-harm and suicide rates in Guyana were one of the worst
globally in 2017 and they have become a high priority for its Ministry of
Public Health, set against the recognition that 79% of suicides occur in low-
to middle-income countries (according to recent WHO statistics). Part of the solution
is for citizens to feel that they can, without stigma or shame, ask for help in
crisis situations, though social and gender coding means (as is the case in
parts of the UK and US) that mental health challenges for men and boys often
goes undetected until it reaches crisis point.
Another element of the solution is to try to reduce, if not
eliminate, social isolation that many advocacy groups identify as the major cause
of depression globally but is often a trigger for suicidal ideations. While no national
healthcare or social services system is expansive enough to prevent all
suicides, the fact that a high prevalence of cases occur in the rural regions
of Guyana where access to health facilities is limited (particularly amongst
farming communities, where a common means of suicide is the ingestion of
agrochemicals), and that mental, neurological and substance abuse disorders are
common in Guyana’s jails, are illustrations of the importance of such
developments.
On World Suicide Prevention Day 2019, following a 500-person
march through the streets of Georgetown, Util Richmond-Thomas delivered a powerful
speech titled “Working Together to Prevent Suicides” at the National Cultural
Centre, focusing on the complex interplay of factors that contribute to mental
health challenges and the need for public-private partnerships to help promote anti-suicide
messages. The statistics about the reduction in documented suicides in Guyana
in 2018 are positive, reducing from 184 suicide-related deaths nationally in
2017 to 141 documented deaths from suicide in 2018 (according to Ministry of
Public Health statistics) out of a population of 747,000. The success of
reducing this prevalence was also evident in the awareness of the young Guyanese
marchers on 10 September on their two-mile march through the streets of
Georgetown. It was an uplifting experience for me, but I was left to wonder
whether the message and resources are getting through to the 25% of Guyanese
living in rural regions away from the Atlantic coastline.
Given that mental health challenges are part of the fabric
of everyday life, only medical interventions via inpatient treatment or a
course of prescribed drugs are easy to document and trace. Unless suicide has a
clear cause it is also difficult to know if a more accessible health centre or
more visible public health information in scattered communities or better job
prospects would make a difference overall. The truth is that all these measures
would help. As other countries have found, no single-step solution to tackling
debilitating mental health conditions is likely to work in the long term, while
drug interventions might only temporarily mask complex underlying issues.
There is a temptation to turn to faith for the answer to the
despair that can sometimes leads to suicide. This faith can take lots of forms.
It can be the faith of organized religion, which is particularly important for
Guyana, a country in which 63% of its citizens (according to the 2012 Census) are
Christian, 25% Hindu and 7% Muslim. It can be faith in a scripture or a faith
in a community of believers, but it is important that it also a faith attuned
to the complex socio-economic pressures that might sometimes strain against
what these three great religions deem as right living. Or, on a secular level,
it can be the faith that life goes on despite hardships, linked to the belief
that all individuals can be agents of change, especially when they share and
work collaboratively.
Reflecting on the
2019 Suicide Prevention Day March in Georgetown, I was particularly struck by a
young University of Guyana student, Dwright Ward, studying in the Department of
Communications, who proudly held the banner “You have the power to say this is
not how my story will end!” I have looked at this photograph a number of times
since that day – a bright young Guyanese student with a powerful message – and
I have thought about both its cultural specificity and its transnational
resonances because it puts into action the 2018 theme of “Young People and
Mental Health in a Changing World”.
On that day of 10 September 2019, so many young Guyanese
were willing to put hope and awareness over their studies and their work. This
image offers hope for an open narrative that can help safeguard mental health,
though it can never guarantee it. And the image offers a powerful symbol for a young
nation that recognizes only a sustained, collaborative and multi-pronged
approach will shift the dial on suicide prevention long term.